The secret of the Rosetta Stone, REDOX Code and the role of HOCl / NaOCl hybrid solutions (data analysis) in the local therapy of chronic wounds
NEW PERSPECTIVE ON AN OLD CONCEPT OF NATURE
DAMIR MARINCIC MD, Quorum Medis Center, St. Gallen SWITZERLAND
INTRODUCTION
We should be using our evolutionary history (living with bacteria and cancer cells) as a basis for gaining insights into what bacteria, biofilms / microbiome, chronic wounds, cancer and general diseases are, why they occur and how we can better treat them. The evolution of nature and species on earth, as well as human history, provides an inexhaustible learning pool about the principles and interrelationships in nature and society. There are so many interesting parallels in evolutionary history that we can learn from. One such “story” is the parallel between the Rosetta Stone, the redox code and the HOCl and NaOCl molecules as part of the redox-redoxome system. Rosetta Stone was written in 196 BC in 2 languages and in 3 writing systems by order of King Ptolemy. The artefact was first found in 1799 in the village of Raschid in Egypt. It took 25 years for the script to be deciphered by two scientists, Egyptologist J.F. Champollion and doctor and physicist Thomas Young. It was crucial that the hieroglyphic code was cracked through the Coptic language (ancient Egyptian language), otherwise we would not have known all that much about Egyptian history. An interesting thing here is a certain connection between Thomas Young and the redox code. He was an all-round genius and the first to give scientific meaning to the word energy, founded on his research into the physics of light. After all, the redox reactions are nothing other than the energy or electron transfer between atoms / molecules, redox pairs with the formation of the redox potential (electro-chemical potential). The redox code also contains a number of physical and chemical “scripts” that we first had to decode. The decoding process had only just started around 100 years ago. During this time, it was possible to explain a large part of this network and its function, yet the mosaic picture still lacks some pieces. It is a stimulating scientific challenge to add the missing pieces and continue the puzzle.
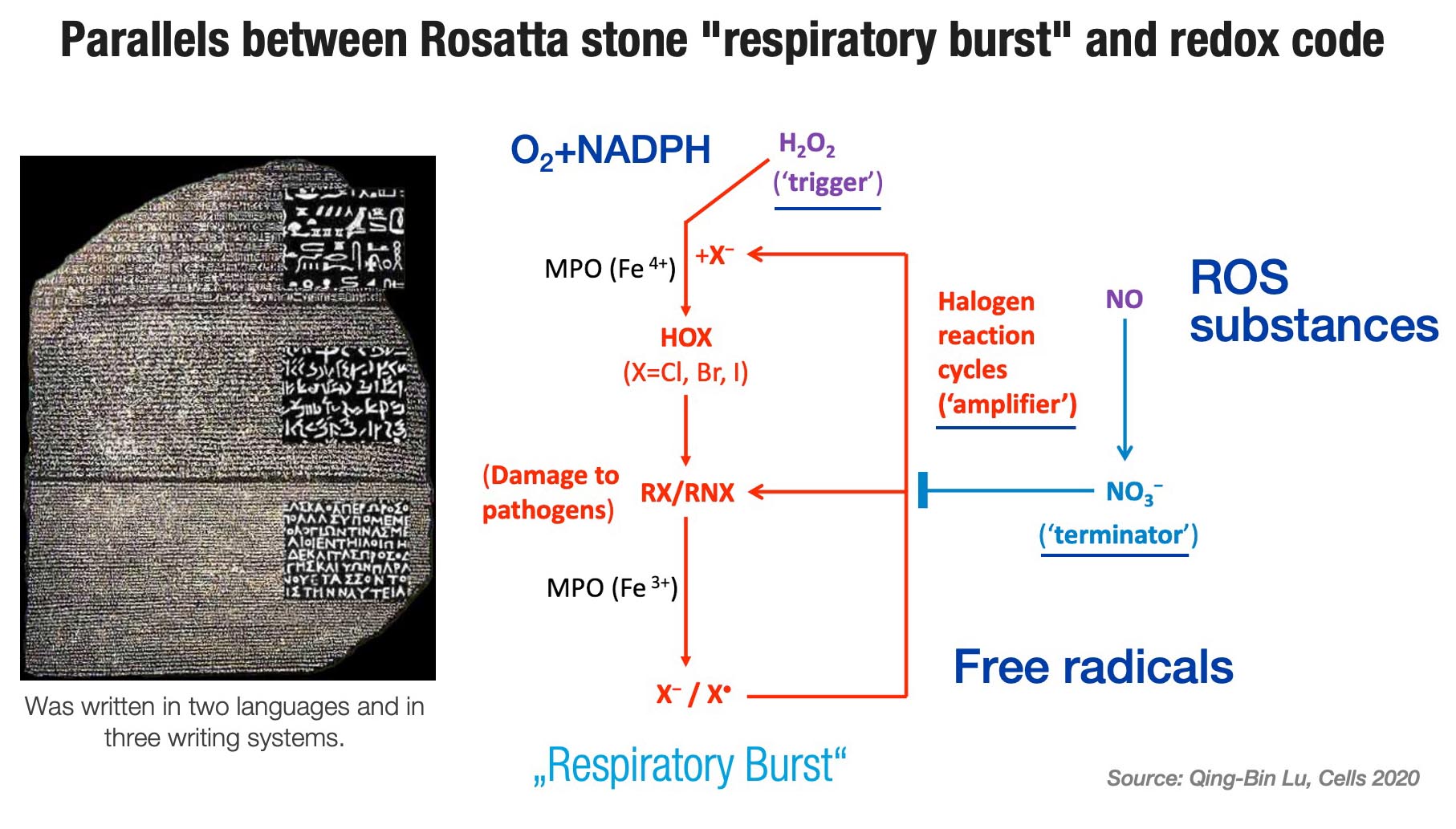
FIG. 1
Rosetta stone is very probably the most important archaeological artefact in the world today. Then again, the redox code is the most important craft of nature/evolution, a complex network system, a foundation of the regulation of cell-biological processes with the stable balance function (steady state) that decides between health-disease and death. The process of life, and in a narrow sense wound healing, can be viewed as the collection, storage and manipulation of free energy. All life on earth is based on redox reactions and electron flow. In essence, life is an electron looking for a home, usually oxygen. In the absence of oxygen, electrons cannot flow, and if electrons do not flow, the amount of nutrients available does not matter. Electron management is the main hallmark of cell biology. It can be concluded from this: no oxygen, no potential, no endogenous electric current (direct current), no cell migration, no healing of wounds. Likewise, oxygen and energy are the preconditions for the temporal-spatial function of the signaling processes, information and communication, since energy and information constitute two irreducible preconditions for our existence. The physical nature of information plays a huge role in biological processes. It is surprising how much physical regulation there is still involved in the natural design of life. The concept of information involves both the quantitative and the qualitative (or semantic) aspects of information, whereby a link is provided between physics and biology.
EVOLUTION OF THE REDOX CODE AND RESPIRATORY BURST
The redox system is a Methuselah concept of nature which was formed about 600 million years ago, following the accumulation of oxygen in the Earth’s atmosphere (only 7%) and transformation of proteo-bacteria into mitochondria during the process of endosymbiosis in eukaryotic cells. Cyanobacteria producing oxygen altered the living conditions and the oxygen concentration of 21%, which was achieved 25 million years ago, marked the breakthrough. Still mature today, and as part of systems biology and complementary codes, the redox code constitutes a complex network with 4 basic principles, involving the buffer system (pro- and antioxidants), similar to the acid-base system, and with its reactive oxygen species (ROS) is an important part of the inherent defense system. During the entire evolution and maturation of the inherent defense system, the endogenous HOCl and NaOCl molecules constitute important parts of this system, just like the other ROS substances (RHS and RNS), physical-chemical derivatives of oxygen, which perform other important functions as signaling molecules (“second messenger”), cell receptors and stimulators of growth factors and stem cells.
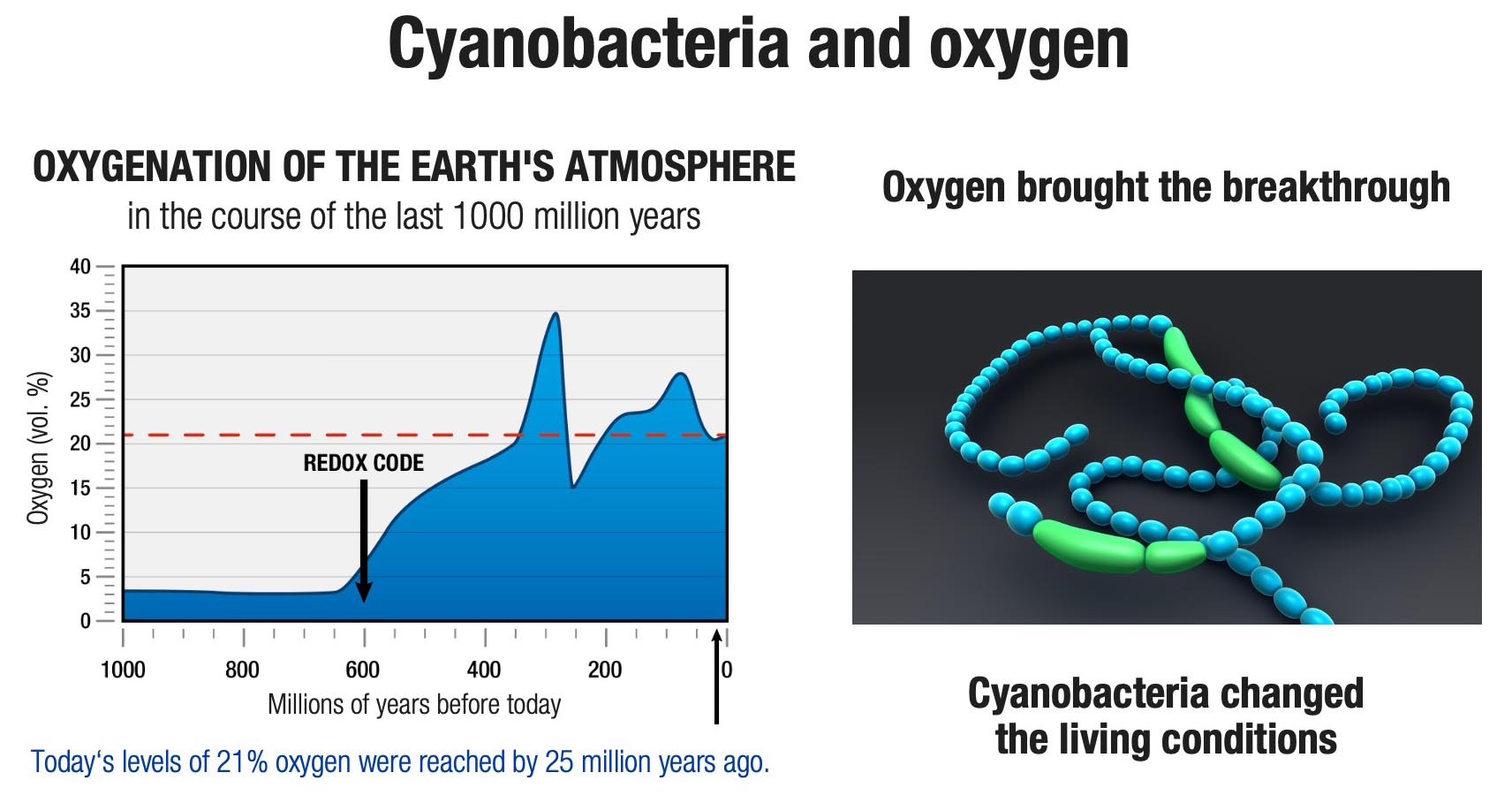
FIG. 2
There is nothing in biology that makes sense except in the light of evolution. Evolution has conserved / retained economic mechanisms and systems that perform many functions, faster or better, with less. In this context, multilevel functionality is one of the first biological principles, and defense is the oldest law of nature. It is in this multilevel functionality that oxygen brings all the pieces of the puzzle back together, since the redox code is richly grounded in a life / cycle dependent on oxygen.
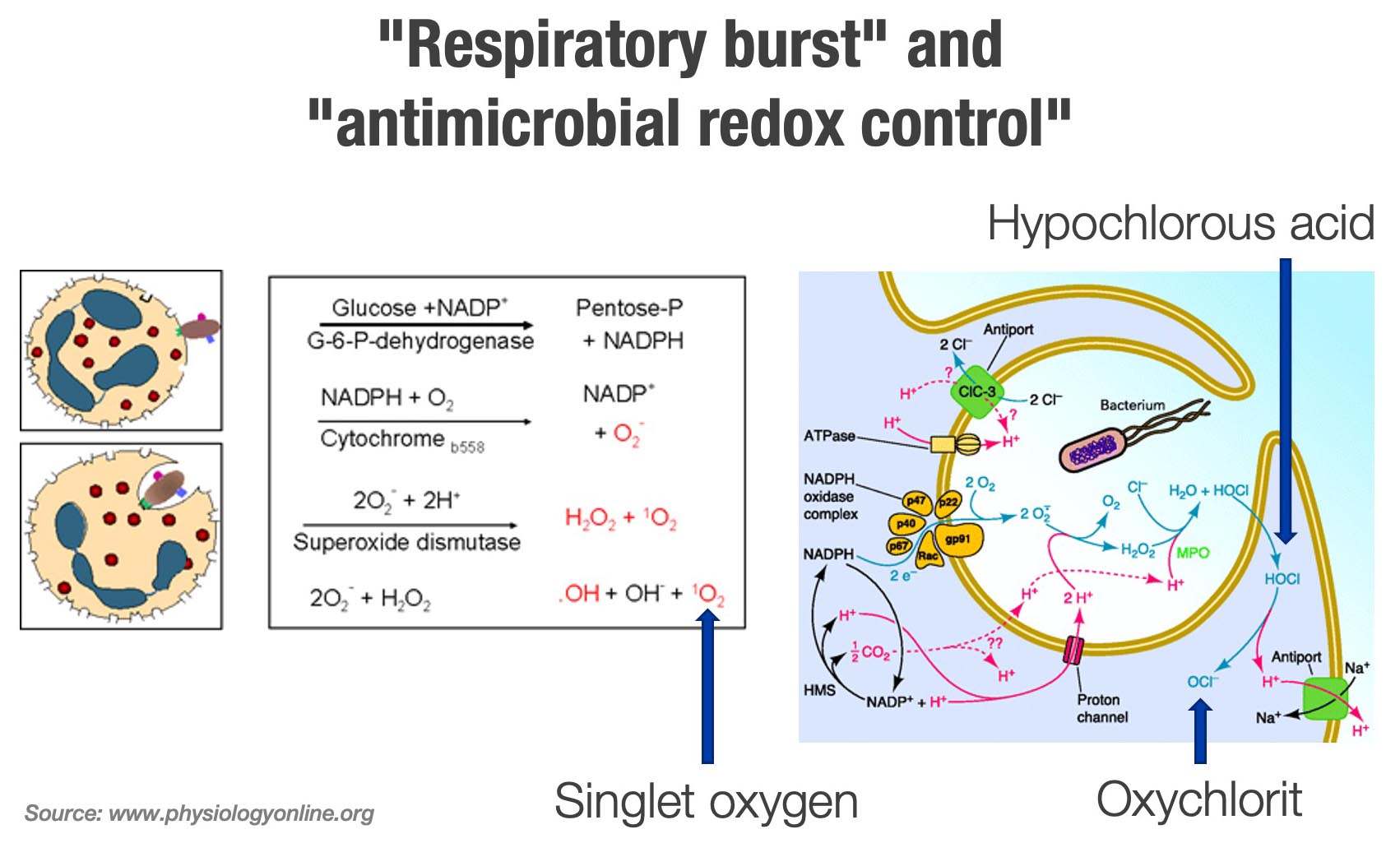
FIG. 3
We can differentiate between primary and secondary Reactive Oxygen Species (ROS). The primary ROS are more signaling molecules, the secondary ones more antimicrobial substances, whereby the primary ones are better controlled through the endogenous antioxidants (A. Kozlov). Within the redox system, the inherent defense system, related to the respiratory burst reactions, is primarily composed of 3 components:
- ROS / NADPH, superoxide and H2O2 acting as activators of signaling pathways and “trigger” molecules.
- RHS (Reactive Halogen Species), MPO and HOCl / NaOCl / OCl anion with reaction cycles (“periodic oscillations”), acting as amplifiers and accelerators (with 100 to 1000 cycles), and
- RNS (Reactive Nitrogen Species), nitric oxide and peroxynitrite with the signaling pathway functioning as a deactivator or terminator of the halogen cycle (see Fig. 1)
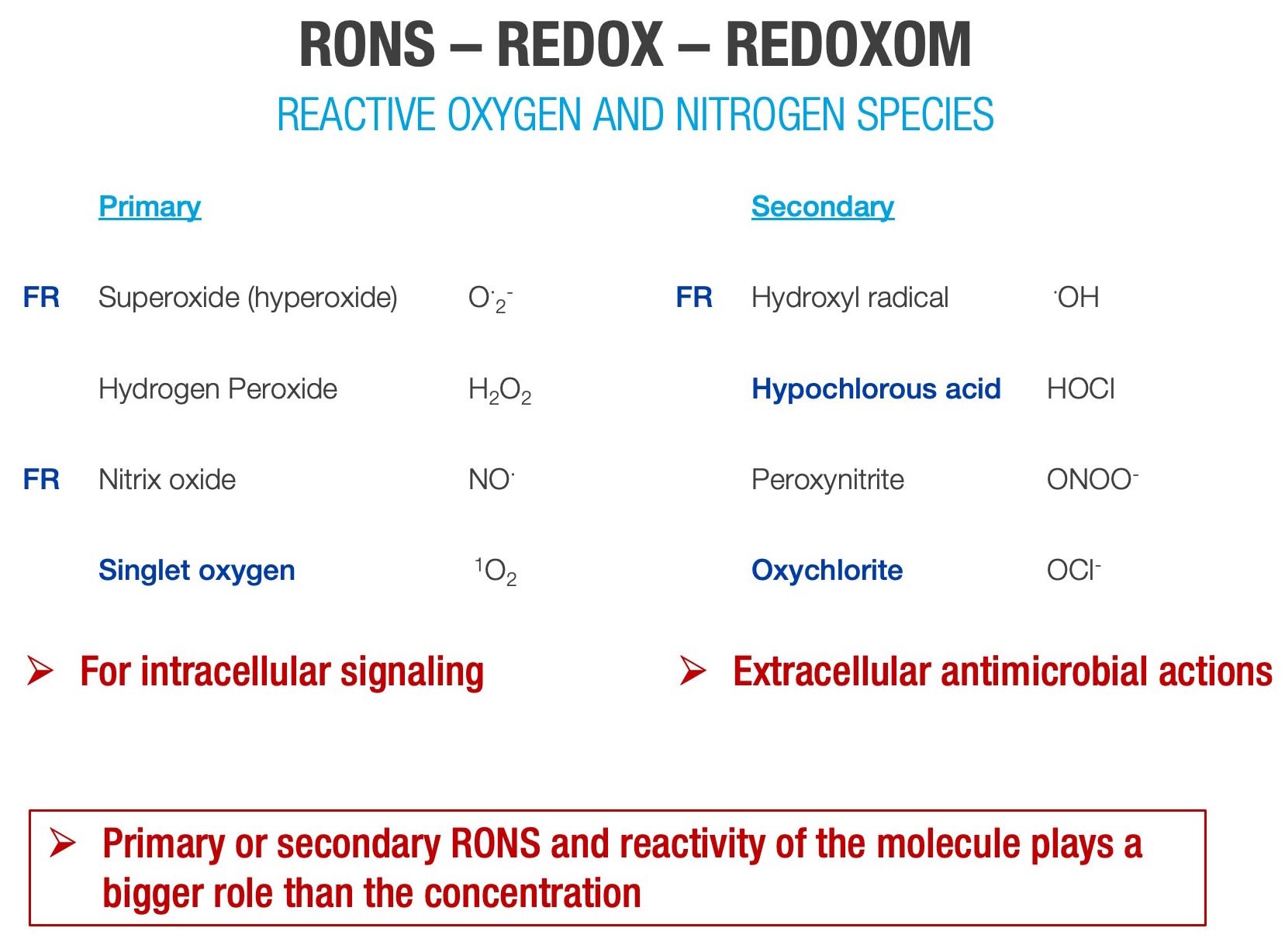
FIG. 4
The redox code is a set of principles defining the positioning of NADH / NADPH and NOX oxidases and other redox systems in space and time in biological systems. Redox systems form redox pairs with their interactions between ROS, RHS and RNS substances. These redox pairs have different voltages, redox potential, allowing electron flow between pairs and therefore the dynamics of the redox reactions. The redox potential is related to the energy that a substance (ROS) has in relation to other substances in terms of electron affinity. The total amount of energy that is required for the multitude of life processes comes from the energy of oxygen and redox reactions. During normal physiological conditions, the redox-optimized ROS balance pertains to the basic and potent evolutionary drive for maximum energy delivery and the crucial ROS-dependent signaling and antimicrobial function of mitochondria (leakage in the electron transport chain), ROS production in neutrophils, macrophages and epithelial cells (“respiratory burst”), as well as the regulation of cell death / apoptosis. The communication process between cells for protection (defense), repair and replacement is the function of redox signaling molecules.
The molecular dynamics of life can best be understood within the framework of the complementary code, its nexus and interactions. Running concurrently with the evolutionary epochs (symbionts) and the emergence of life, it was absolutely necessary to develop systems for controlling physical, chemical, molecular and cellular networks with the complementary code, as the molecular logic of life. The Nobel Prize winner for chemistry in 1967 Manfred Eigen was even of the opinion: “Our ancestors were originally not living beings, but processes (physical, chemical, biological). He influenced the physics of biology and concept of evolutionary dynamics, also known as “quasi-species” theory.
The complementary codes control and are regulators of many different functions. Cell biology is in fact regulated by the complex networks. We are in the process of dedarwinification, moving from the tree of life towards the web of life, shifting towards a dynamic interaction network at molecular, cellular and extra-cellular levels (symbionts). Here, redox, epigenetic and symbiotic codes are eminently important for immune defense, gene expression and tissue repair/regeneration, as well as for wound healing processes. The redox code, which is made up of 4 principles, is at the core of these nexus reactions:
- Energetic and metabolic organization
- Connection between metabolism and structure, especially of proteinse
- Redox “sensing” (oxygen) and redox “signaling” (ROS) and the spatio-temporal differentiation of redox metabolism, where ROS play an “interface” role
- Redox systems adapt to our environment and also to the micro-environment in the wound (epigenetic code) where the ROS substances act as receptors and regulate the expression of genes.
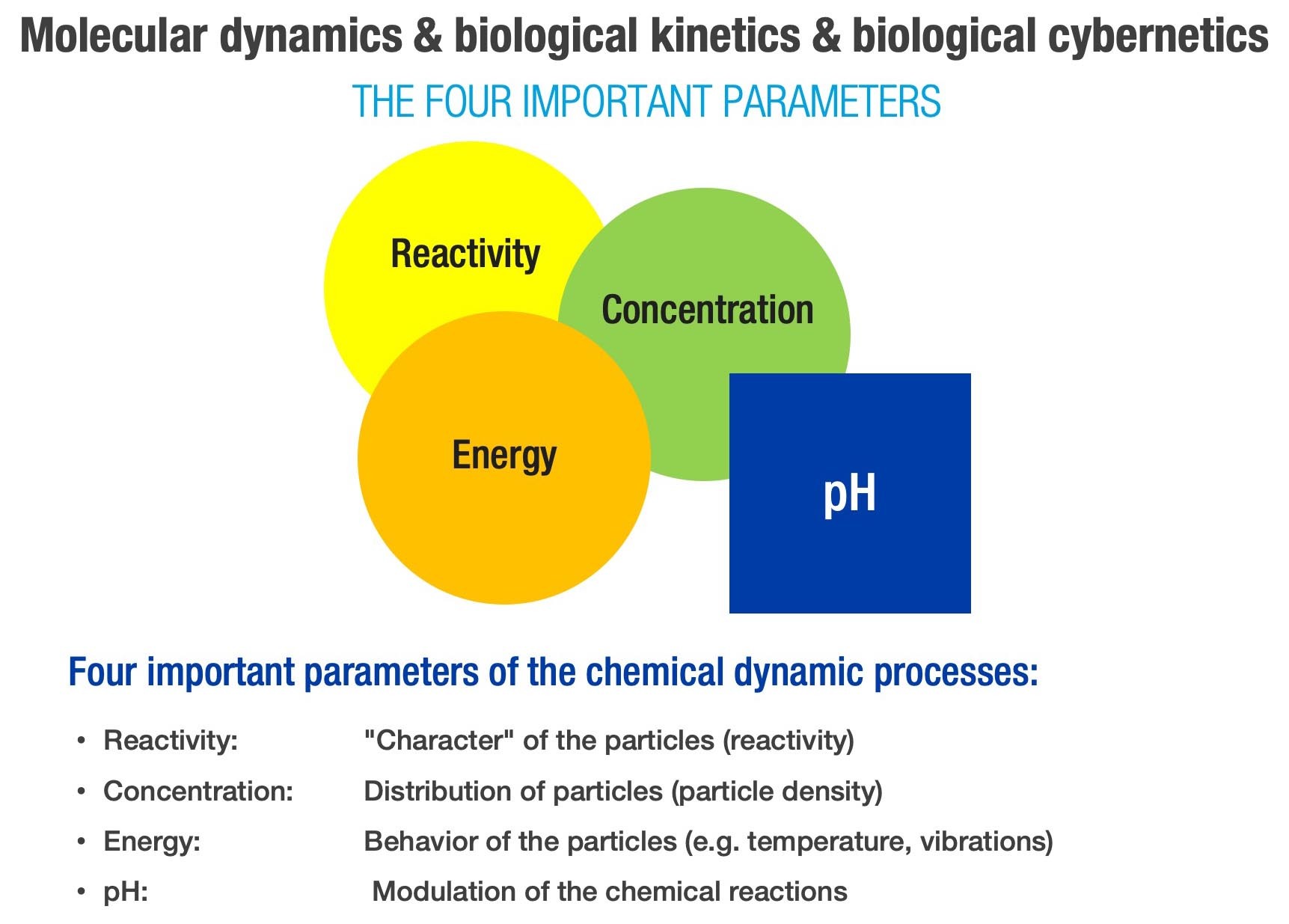
FIG. 5
In spite of the history of the redox phenomenon and “respiratory burst” cascades in the defense cells of the inherent immune system dating back millions of years, the traces and significance of the “respiratory / oxidative burst” were only discovered almost 100 years ago. This was described by Baldridge and Gerard in 1933. Rossi and Zatt found in 1964 that the enzyme NADPH oxidase triggers the “respiratory burst” process in neutrophils. S. J. Klebenoff found in Seattle in 1967 that MPO-H2O2-Halids-H2-chloride ion complex (and thiocyanate) functioned as a powerful anti-microbial system in neutrophils and macrophages. Babior, Kipnes and Curnutte reported in 1973 that superoxide anion is the first product of the “respiratory burst” process. Many secrets of this natural phenomenon and its function have been revealed in the last 50 years and cell physics and cell biology have been made much more comprehensible.
The ROS substances / molecules are ubiquitously produced, in defense cells (neutrophils, macrophages), epithelial cells and in mitochondria during leakage along the electron transport chain (ETC). Since the electrons for ATP synthesis are not transported further, they are redirected by NADH oxidase directly to oxygen with the formation of the superoxide radical. The mitochondria have retained their dual evolutionarily anchored function, namely to produce ATP and ROS, to this day. This process of mitohormesis (adaptation and tolerance) involving the hormetic effect-dose curve, also occurs in macrophages with the reprogramming between pro-oxidative and pro-reparative phase (OXPHOS) in the process of healing wounds (S. Willenberg et al., Cell Metabolism, 2021). Research conducted by J. Jantsch suggests that cutaneous salt/NaCl storage and the hypertonic milieu (hyperosmolarity) promotes macrophage-driven defense functioning. Parallels are found between the process of Oxidative Phosphorylation (OXPHOS) in mitochondria and the “respiratory / oxidative burst” process in defense cells / neutrophils. This is impressive confirmation that defense is the oldest law of nature.
THE HISTORY OF EXOGENOUS HOCl / NaOCl HYBRID SUBSTANCES IN THE TREATING OF WOUNDS
In comparison to endogenous ROS substances, which are produced in neutrophils, macrophages, epithelial cells and mitochondria, the “exogenous” HOCl and NaOCl molecules or HOCl / NaOCl hybrid solutions only have a relatively short history dating back 235 years. This starts in 1785 (40 years before the Rosetta Stone was deciphered) with the chemical production of NaOCl solution by Barthollet / Eau de Barthollet. Some 7 years later, in 1792, KOCl / potassium hypochlorite solution was also chemically extracted, in the suburb of Paris, Javel, Eau de Javel, solution which to this day is mistakenly considered as sodium hypochlorite. Eau de Labaraque, a mixture of KOCl and NaOCl, also obtained by the chemical process, appeared on the market 90 years later, in 1882. It was not until 125 years ago, in 1895, that hypochlorite and hypochlorous acid were first extracted through the electro-chemical activation / ECA (electrolysis) of a salt solution by Walter Nernst (Nobel Prize for Chemistry and Physics 1920), known also for the Nernst equation, which makes it possible to calculate the redox potential. The ECA process for the extraction of HOCl / NaOCl hybrid solutions has fallen into obscurity for decades, not least because of its chemical instability. Carell and Dakin introduced a Na-hypochlorite solution (0.5-1.0 %) to the market in 1915 / 1916 during the First World War, known as Dakin’s solution for the local treatment of infected wounds in injured soldiers, however this was also chemically extracted and buffered due to instability. As with the endogenous ROS / RHS substances, the exogenous HOCl / NaOCl / OCl anion molecules also potentiate the cyclic reactions of the “respiratory burst” process and consequently exercise a significant antimicrobial effect as part of the immune response. The scientific team of the Department of Biochemistry, University of Bochum, Germany, produced cinematic evidence in 2018 that our immune system uses chlorine bleach (HOCl / NaOCl / OCl) to kill bacteria. The amount / concentration of the ROS / RHS substances should not exceed that of the endogenous substances, whereby the inherent reactivity of a substance takes on a more important role than the concentration. Reactivity of hypochlorous acid / HOCl is approx. 80 times higher than that of hypochlorite / NaOCl), yet more toxic to cells as a result, since it is also considered a precursor of free radicals (A. Panasenko).
A. Fleming’s discovery of penicillin in 1928 and its introduction into clinical use 10-15 years later caused antimicrobials and antiseptics to be overlooked. Some 40 years later, roughly in the early-mid 80s, and with the increase in bacterial resistance due to inadequate antibiotic use, which Fleming predicted relatively early on, the significance of antiseptics increased again.
CONSENSUS GUIDELINES vs. FACTS AND OPINIONS
The approval of antimicrobial products, including HOCl / NaOCl solutions for the topical treatment of chronic non-healing wounds, has skyrocketed since that time, along with the marketing propaganda to go with it. Consensus statements and therapy guidelines were distributed, whereby, according to information from the literature, 2/3 of these were / are organized and paid for by participating companies, in each case to push their product to the top. We have had consensus papers published in German-speaking countries since about 2004 on antiseptics in local wound treatment featuring almost always the same panelists, who have only dared to present and evaluate the HOCl / NaOCl hybrid solutions as equivalent to the octenidine-PHMB-povidone-iodine products since 2018 / 2019. Topic oxygen therapy (TOT) has been forgotten in these guidelines, despite the recommendation and guideline for TOT therapy issued by EWMA in May 2017. In this context, it is known that without oxygen, no oxygen derivatives / ROS substances can be formed, no oxygen gradient can be built up in the tissue and in the cell (pO2) and no physically dissolved oxygen, which cells need for their work and metabolic processes, is available.
A normally functioning cell needs about 1012 O2 molecules per day. A damaged cell even more. The tissue of chronic wounds is hypoxic, acidotic, low in energy, lacking bio-electricity (current), low in minerals (lacking electrical conductivity) and low in redox potential, which results in higher bacterial persistence and resistance. Neutrophils stop migrating in hypoxic and acidotic tissue, as well as in weak endogenous DC. Electrical current, “injury current” is a overriding signal for cell migration and wound healing (Min Zhao). In order for a wound to heal, the body’s metabolism must raise energy production by 20% for clean wounds and 50% for infected wounds. In addition, local overtreatment (“overuse therapy”) of chronic wounds makes the wound stagnant and “sicker”, lower in energy and less likely to heal. It is not more therapy that leads to improvement, but adequate, targeted therapy. All this needs to be corrected in our therapy concepts if we want the stagnant / non-healing wounds to move in the direction of healing. Eradication of pathogenic bacteria and wound biofilms is not enough. It makes the work / therapy easier, but it is only a half-measure.
Due to the “bias” elements in consensus / guidelines papers, generally speaking, they should not be followed “tel quel” and implemented only “cum grano salis”. The conclusions and justifications regarding the application of certain local wound products sometimes seem like the Oracle of Delphi, like an ambiguous prophecy, therapeutic advice, which can be rather mysterious, so that the oracle can become a debacle. The prophetic high priestess Pythia in the temple of Apollo was put into a trance state due to the lack of oxygen (as in chronic wounds) as a result of natural gas poisoning (geologically proven in Delphi). That is why (current theory) she made ambiguous prophecies. What the High Priestess was doing then, “Big Pharma” is now doing consciously and the danger of a Pharma-geddon is ever closer. There are unfortunately plenty of examples.
There is a gradual shift from optimism to disillusionment when it comes to the commitment to transparency in the medical-industrial complex. Scientific honesty ought to be the hallmark of any experiment, whether in fundamental or clinical research, yet the landscape of scientific publications is changing. The number of scientific journals explodes (over 20,000) and the quality/power of publications erodes. It may rhyme, but it doesn’t make sense (Gottfried Schatz: “The risks of playing safe”). On the other hand, the quantity of “evidence bias medicine” publications and “peer review fraud” cases keeps rising. And the tail continues to wag the dog as we are creating something that is of minor importance to the wound healing processes. This is the truth of which we are all aware, but which we do not want to talk about, even though we are dealing with the elephant (problem) in the room.
EVIDENCE-BASED MEDICINE, A MOVEMENT IN CRISIS?
Similarly, “Evidence-Based Medicine” / EBM with the integration triad according to David Sackett (1990): combining the best available evidence with the clinical experience / knowledge and the values and expectations of the patient, is primarily aimed at the specific diagnoses and is not always applicable to the individual patient. Commenting on this, David Sackett himself once said: Practice is threatened with being tyrannized by evidence.
Facts and opinions serve complementary functions in research and clinical decision-making, while the good thing about facts is that they can be verified. In doing so, we need to contemplate the half-life of facts, the subjectivity of (one’s) opinions and the relativity of being wrong. About half what you learn in medical school will be shown to be either completely wrong or out of date within 5 years: The problem is that no one can tell which half that is (David Sackett, 1996). The processes of education and advanced training are not just about learning facts; they are much more about training the mind to reflect on the facts (Albert Einstein).
An established opinion is not always the right one: de-construction and re-construction of theories is part of the scientific process, since facts also have their half-life. There is nothing in the history of life that is more constant than change (Charles Darwin). Medical science is accelerating and progressing, but we are stagnating and sometimes refuse to incorporate new findings into our therapeutic concepts. After all, it is not what we knew before that takes us forward, but only what we never knew. For he who remains on the coast cannot discover a new ocean (F. Magellan).
Evolution is the most fundamental science (evolutionary biology) of medicine and the natural laws of evolutionary heritage point us in the right direction. Paracelsus, the first modern wound doctor, said 500 years ago: “Nature does not follow you, you have to follow it. Wounds and injuries have been healed in accordance with certain laws since the beginning of time, and will certainly continue to do so tomorrow”. How brilliant / ingenious, even though he did not know at the time that these were the natural laws of the redox system and the functions of the ROS signaling pathways for the repair and healing processes.
This is why, without understanding fundamental scientific processes, understanding mechanisms of action, it is not possible to develop targeted, success-oriented therapy concepts, or as Max Planck put it: “Understanding must precede application”. Knowledge comes by taking things apart: ANALYSIS, but wisdom is created by putting things together: SYNTHESIS (J.A. Morrison). This is why it is recommended to first analyze which local therapeutics are used for the treatment of chronic non-healing wounds and pathogenic biofilms, as well as for the support of healing processes, in order to subsequently look at this evidence synthetically and put it together in order to orientate towards the group of HOCl / NaOCl hybrid products.

FIG. 6
“MODERN” LOCAL WOUND THERAPY, NEW PERSPECTIVE ON AN OLD CONCEPT OF NATURE
There are basically 2 groups of local therapeutics used in local wound therapy: xenobiotics and endo / eubiotics. These are joined by the unavoidable “adjuvants”, both inert and active wound dressings and bandages (estimated to be several thousand products on the market), not least for hygienic reasons. Research in recent years and the development of biotechnology have brought some new local wound therapeutics to the threshold of clinical use. Antibiotics are rarely used in local wound therapy and are no longer recommended because of the danger of developing resistance. Xenobiotics are substances that are foreign to our cells, mostly large molecules (polymers) with the potential to trigger immune reactions (allergic). This group is very heterogeneous. Prolonged use, especially of sublethal doses (for microorganisms), may result in the development of bacterial resistance. Cross-resistance between these substances has already become known, e.g. chlorhexidine. To this end, they cannot be signaling molecules and consequently no direct active support of the healing process, secondarily perhaps due to their antimicrobial effect. Some wound products belonging to the group of xenobiotics and some metals belong to the group of oligodynamic (low potency) substances with prolonged onset of effect and thereby increased cell toxic potential, meaning that some of them need the help of surfactants / detergents in order to achieve a better effect by shortening the soaking time.
FIG. 7
The Eubiotics group predominantly make the HOCl / NaOCl substances / solutions / gels. These small reactive, pro-oxidant molecules replicate an endogenous antimicrobial mechanism within the framework of oxidative bursting, like in our defense cells. ROS substances have made a long “road to Damascus” over the last 50 years, making the transformation from Saul to Paul. They are primarily the “shielding” molecules, or an effect (response) to the cell lesion or disease instead of being primarily the cause, since it is the damaged tissue (cells) that triggers the production of the ROS substances. High concentrations of particularly secondary reactive oxygen species, which have no protection from endogenous enzymatic antioxidants, may cause the stress reaction and tissue damage. Just like singlet oxygen, they are the oxymoron molecules. When in balance with the antioxidants, we speak of eustress, because it is better for the tissues/body to have more Reactive Oxygen Species (ROS) than to have more antioxidants (Michael Ristow), which has also been shown in some clinical cancer studies.
If detailed data analysis is carried out on the production technology, concentration of ingredients and physico-chemical parameters, it has to be noted that the HOCl / NaOCl hybrid group also shows a level of heterogeneity. This heterogeneity is reflected primarily in the physico-chemical parameters (not in technology, biological or clinical factors), but also in the clinical “Efficacy-Safety-Effectiveness” results, factors which determine the equivalence and/or discrepancy (deviation from the ideal state) within the group. Over 90% of HOCl / NaOCl products for local wound therapy are derived by ECA technology, less chemically and stabilized by buffers. Concentration of the components, pH-value and other physico-chemical parameters may be quite different, resulting in different product complexes, as is clearly shown by the study situation and the literature study.
Concentration of ingredients / ROS plays a contributory role from various aspects. The degradation kinetics are faster at low HOCl / NaOCl concentration, acidic pH value and higher protein concentration in the wound resulting in a weaker effect accordingly. When the HOCl / NaOCl concentration is below 0.01 % (100 ppm), the “second messenger” molecule di-cy-GMP in biofilms is stimulated to form EPS / matrix, which is also associated with resistance to therapy. There is also a risk of developing bacterial tolerance at low, sublethal concentrations. With a HOCl / NaOCl concentration between 0.01-0.08 %, the antibacterial effect on planktonic bacteria is effective in vitro between 4-6 log10, however in vivo, much weaker in the wound, only 1-2.5 log10 (A. L. Severing et al., and G. Kammerlander, O. Assandian, 2018). This also suggests that clinical evidence is more important than in vitro data. Laboratory tests only simulate clinical conditions and mostly do not correlate with clinical performance.
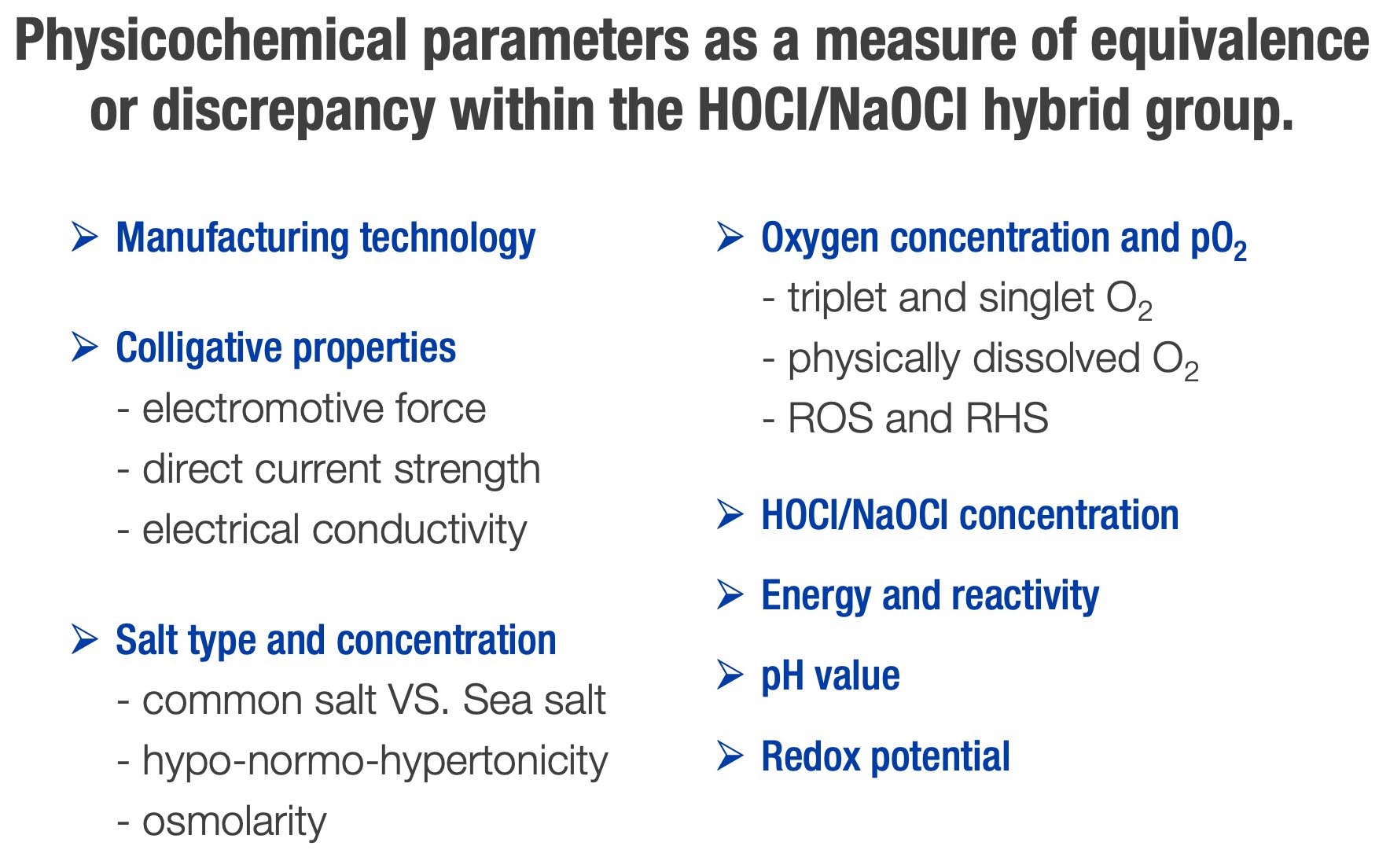
FIG. 8
It is worth noting at this point that a so-called bioelectrical / electro-bioceutical effect also takes place in the body tissue, which is somewhat similar to ECA. Studies have shown that chloride is an important parameter that has been proven to increase the antimicrobial effect of the endogenous electric current. If a direct current is established in vivo, where chloride is abundant, the generation of chlorine (RHS) becomes an inevitable consequence. To put it another way, micro-electrolysis takes place in the tissue (C. R. Kruse et al., 2017).
We are alkaline organisms and life originated in the primordial sea, in an alkaline pH environment and hypertonic salt solution, yet the primordial sea was the experimental laboratory of evolution for millions of years. Most structures in the cell, in tissue, also function optimally in a neutral-base range. The pH with its spectrum acts as a modulating factor of chemical reactions and coordinator of physico-chemical parameters (S. Huijghebaert et al. 2020). The adequate pH (acidic or alkaline) also controls the cascade sequence of the oxidative burst process. The temporal-spatial pH dynamics in chronic wounds are multifactorial and fluctuating, just like the wound microbiome. The pH value influences the interaction between physico-chemical parameters, whereby the salt prevents acidification of the solution/tissue and exerts a supporting influence on the electrical conductivity and the redox potential. Bacteria are at their best in the pH range for growth, as are the antiseptics for efficacy, whereby these can influence the superficial pH value of the wounds. What is important here is to realize that in a chronic wound a reciprocal molecular dynamic and a struggle between different “participants” and a lack of “building material”, but also chaos, prevails. In terms of therapy, the aim is to restore order to these stochastic relationships in the wound tissue and to restore the physiological milieu and orderly, non-random processes.
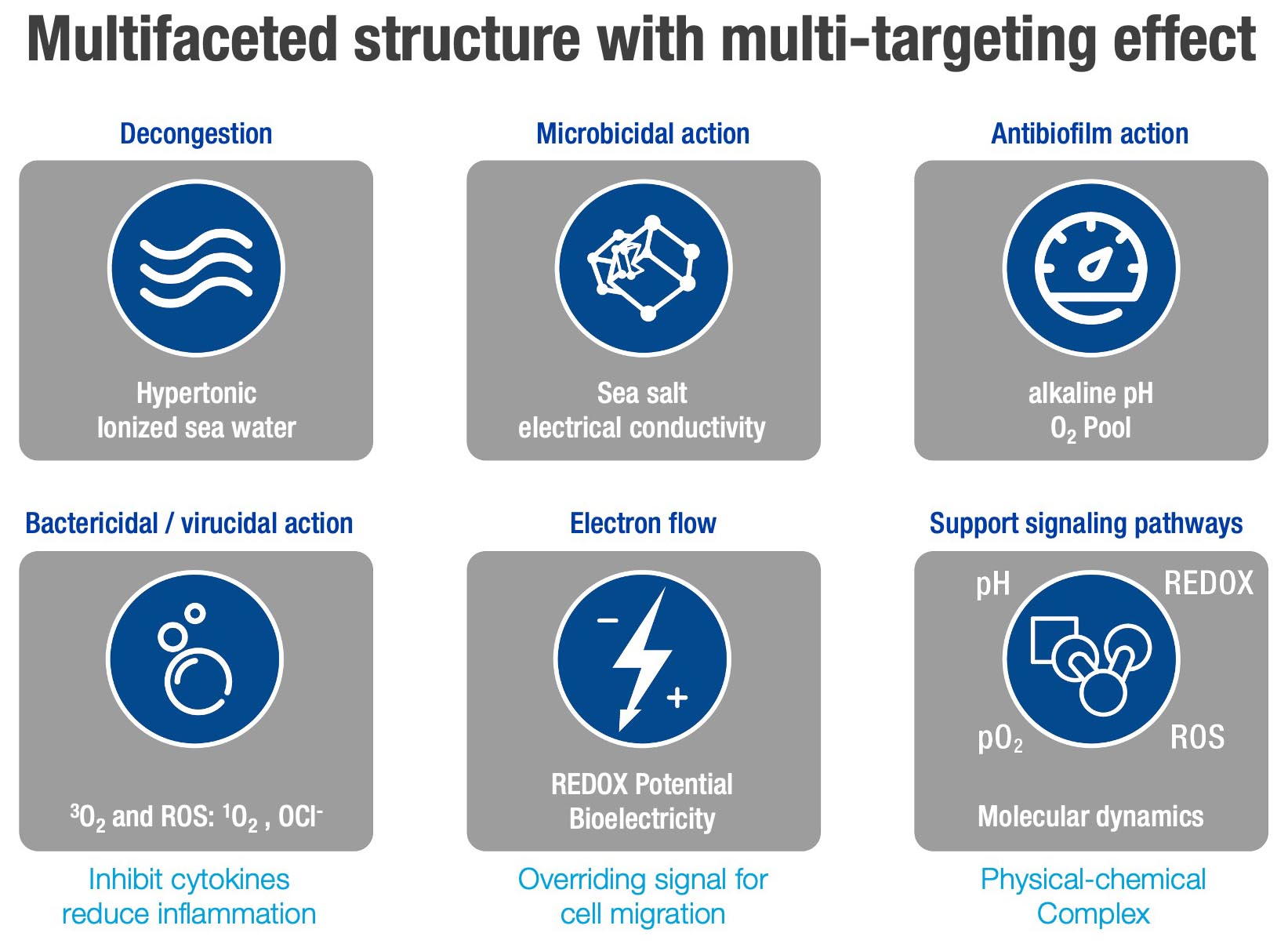
FIG. 9
Chronic wounds (as well as tumor wounds / ulcers) have a low energy, are hypoxic, acidotic, mineral deficient and weak in current (injury current) with a low redox potential. Tumors are wounds that do not heal. The wound healing process, chronic fibrosis, cancer progression and metastasis use, to some extent, similar signaling pathways, which is why we also speak of the WHFC triad. It has been known since research on tumor cells 100 years ago by the Nobel Prize winner Otto Warburg that tumor cells shift from respiration to fermentation (so-called aerobic glycolysis). Back then, Otto Warburg already said that no tumor and no disease can develop in an oxygenated, alkaline and mineralized (Linus Pauling) tissue.
This is why it is important to alter this pathological state therapeutically. There is a struggle for oxygen and energy in chronic wounds with infections, biofilms and chronic inflammation, as well as an ongoing attempt to transform the pathological milieu back into the physiological state. Failure to win this battle causes the wound to stagnate and not heal. The “trigger” factors and “support” mechanisms, the stimulation of signaling pathways does not lie in the armamentarium of xenobiotics, rather it is the weapon and mode of action of a sophisticated “Oxygen-ROS-Redox” complex with its physical-energetic potential and balanced physical-chemical parameters. This complex would ideally have to follow the principles of the redox code and work within the framework of its network. And this is precisely where the roots of the differences and discrepancies in the mode of action, safety and effectiveness / usefulness within the HOCl / NaOCl hybrid group lie, because not all of them can perform the three following strategic-tactical therapeutic steps:
- 1. Delivery of oxygen (singlet and triplet) and energy, correction of hypoxia and acidosis with pH modulation of enzymatic reactions. There is competition in chronic wounds between immune cells (respiratory burst), mitochondria (ATP synthesis), bacteria in biofilms, repair cells (keratinocytes and fibroblasts) and growth factors, whereby the processes of the signaling pathways also consume energy. The chronic inflammatory state associated with non-healing wounds is almost always accompanied by hypoxia, with the hypoxia and acidosis blocking the migration of neutrophils and macrophages.
- 2. Supply of electrolytic, serum-like, alkaline-ionized and hypertonic (hyperosmolar) sea salt solution for changing the pathological wound milieu (chronic wound fluid) into the physiological state, which leads to the dissolution of biofilms and acceleration of the healing processes. This also shows how important the epigenetic code, even in the microclimate of the wound (wound biotope), for gene expression and re-establishment of the physiological state in the tissue is.
- 3. Reduction of “bioburden”, biofilms, inflammation and wound infection by the ROS substances ((HOCl / NaOCl / OCl anion and singlet oxygen), as well as by the redox potential, electrical conductivity, basic pH (blockade of “quorum sensing”) and also by sea salt and the hyperosmolarity, within the meaning of the synergistic antimicrobial effect, as in the ActiMaris complex.
Biofilms in chronic wounds pose a real therapeutic challenge. The literature and clinical experience indicate that they are found in 85-90% of wounds, whereby the wound microbiome can and usually does change during the different phases of the wound. A stable wound microbiome usually indicates that the wound is resistant to therapy. The biofilms exhibit very active molecular and electrical dynamics, in keeping with the motto: “Stay in touch, while on the go”. The biofilms have a 3D architecture and are like “Facebook” for bacteria with a multi-level, integrated communication system (M. Williams). The formation of biofilms in the wound begins with a pathological wound milieu and adhesion of planktonic cells with the formation of microcolonies. The biofilms do not produce the pathological milieu, but they grow because they find a “good” nutrient medium to grow. This is followed by what is often forgotten electroattraction with electrical signals across the potassium channels with migration via modulation of the tumbling frequency to the biofilm center. Following biofilm maturation and diffusion and penetration into the wound tissue, dispersion of the sessile bacteria back into planktonic form takes place. This is almost a “perpetuum mobile”, and the reason for why anti-biofilm therapy is a therapeutic crux. The first step in eradicating the biofilms on chronic wounds is to destroy their chemical (with alkaline pH above 8.2 and blockade of N-acyl homoserine lactone / “quorum sensing”) and electrical (redox potential, electrical conductivity) communication so as to kill the planktonic bacteria released by the ROS substances. In order to achieve a successful anti-biofilm effect, the biofilm matrix must also be destroyed. Chemical and electrical action means that more than half the work is done, but not all of it. A hypertonic saline solution and the power of high hyperosmolarity are still required in order to physically degrade matrices. The need for a strong antimicrobial effect persists, yet the concentrations/doses for an efficient anti-microbial effect, based on research, must be at least 10-100 times, up to 1000 times, higher than for the killing of planktonic bacteria. The conclusion to be drawn from this argumentation and data analysis can only be one, and that is that only a limited number of products can achieve the goal. Based on deductive principles and essential characteristics of individual HOCl / NaOCl hybrid products and the evidence situation (“basic science and clinical experience”), it should not be difficult to decide on the selection.
The local therapy concept is quite simple in principle and can be summarized within the framework of a SLOGANS:
SUPPLY the tissue with oxygen / ROS and energy
ENSURE a healthy environment for the wound
REDUCE the microbial and tissue burden, as well as the therapeutic overload
SPEAK the LANGUAGE of the cells and ENHANCE their repair and signaling pathways.
The excellent expert in redox biology Chandan K. Sen expressed the formula for solving this problem in the damaged tissue/wound as follows: “Let there be oxygen, let’s charge the cell battery and let’s walk the talk of cells, because the oxygen put all the pieces together again”.
The HOCl / NaOCl hybrid products can be fundamentally divided into 4 groups based on the discrepancies and deviations from the ideal status of the physico-chemical parameters and concentrations, as shown in Figure 9.
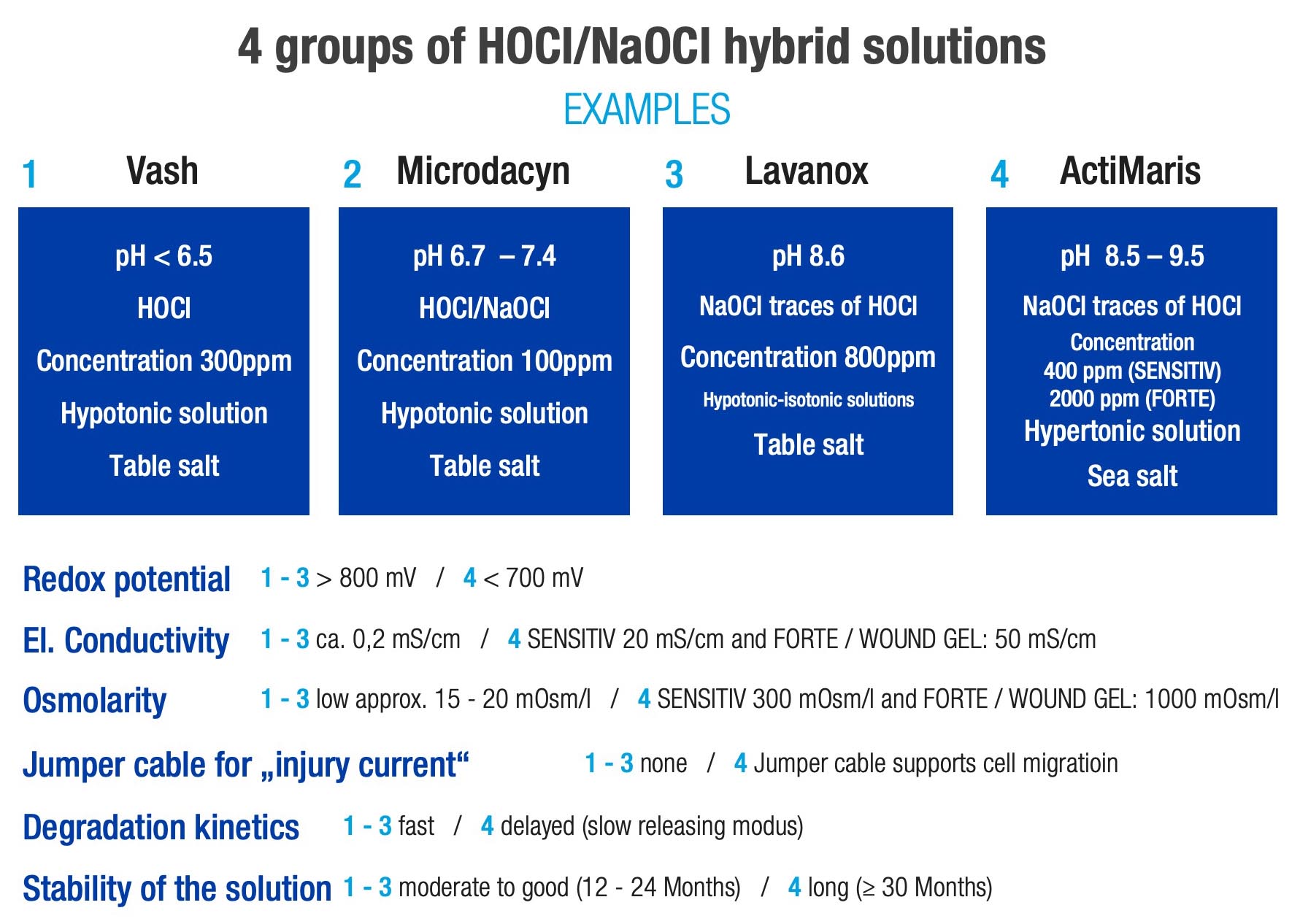
FIG. 10
It is the 6 parameters plus the concentration of the ROS substances and the type and concentration of the salt that warrant this classification and the formation of a separate 4th group solely for the ActiMaris complex. ActiMaris products form the only local wound products with 2-“power level” action (Sensitive and Forte) and 3-“speed level”, according to onset of action time (onset and duration of action). ActiMaris Forte (10-60 seconds), ActiMaris Sensitive (1-10 minutes) and the ActiMaris Gel with the “slow releasing” mode and prolonged action due to higher viscosity, 3% sea salt and high alkaline pH. These variable properties can be adapted well to many kinds of acute and chronic wounds and in accordance with the healing phases as well as clinical situations. Such therapeutic scope cannot be found in any of the local wound products / solutions and gels that are currently on the market. This “multilevel”, “multifunctionality” and “multitarget” concept with 3 (6) products, yet with an equivalent complex, also signifies a paradigm shift in the local therapy of acute and chronic, non-healing wounds with various aetiologies, as well as inflammatory and infectious skin and mucous membrane processes. In contrast to the “unitarget” therapy, the optimized, “multitarget” treatment is able to achieve a stronger clinical effect, reduce cell toxicity and impede or completely prevent the development of resistance. The concept is currently being re-examined in an ongoing clinical trial, “Comparative Effectiveness Research” in accordance with standard EN ISO 14155. The guiding concept behind this is in the sense of Albert Einstein’s aphorism: “Strive not to be a success, but rather to be of value”, specifically in this case, for the clinical results from which our patients can derive therapeutic benefit.
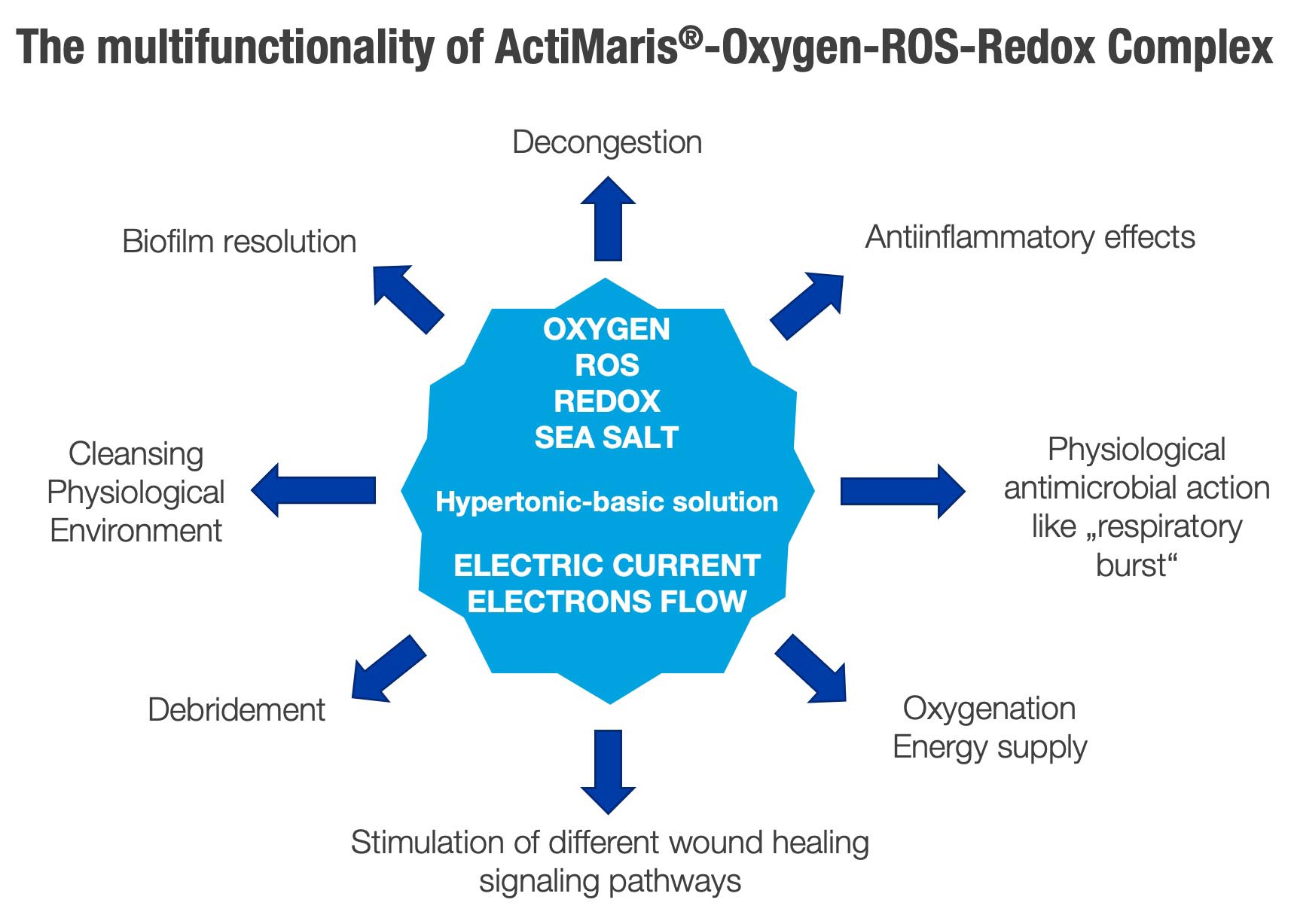
FIG. 11
Wound management is a matter of knowledge, wisdom and clinical experience, but sometimes contaminated with different interests and points of view. For example, symbolically as a wound cleanser, decolonizer (“breaking the point of pathogenecity”) and local wound treatment agent, the ActiMaris complex guides us on the path we should follow with coordinates of near-perfect performance. After all, as Confucius said 2500 years ago: The journey (learning process) is the destination. What matters is not so much what we achieve at the end of the journey, but what we experience, learn and which values / results we create during the journey. There is no value in taking a shortcut on this path, as it can misguide us, since the problems with the therapy of non-healing wounds cannot be solved with the same mindset that created them.



{kind=link}
{kind=link}